Down Syndrome Abstract
of the Month: Aug 2001
Homocysteine metabolism in children with down syndrome: in vitro modulation
Pogribna M, Melnyk S, Pogribny I, Chango A, Yi P, James SJ
Am J Hum Genet 2001 Jul;69(1):88-95
Division of Biochemical Toxicology, Food and Drug Administration National Center for Toxicological Research, Jefferson, Ark., USA
Abstract:
The gene for cystathionine beta-synthase (CBS) is located on chromosome 21 and is overexpressed in children with Down syndrome (DS), or trisomy 21. The dual purpose of the present study was to evaluate the impact of overexpression of the CBS gene on homocysteine metabolism in children with DS and to determine whether the supplementation of trisomy 21 lymphoblasts in vitro with selected nutrients would shift the genetically induced metabolic imbalance. Plasma samples were obtained from 42 children with karyotypically confirmed full trisomy 21 and from 36 normal siblings (mean age 7.4 years). Metabolites involved in homocysteine metabolism were measured and compared to those of normal siblings used as controls. Lymphocyte DNA methylation status was determined as a functional endpoint. The results indicated that plasma levels of homocysteine, methionine, S-adenosylhomocysteine, and S-adenosylmethionine were all significantly decreased in children with DS and that their lymphocyte DNA was hypermethylated relative to that in normal siblings. Plasma levels of cystathionine and cysteine were significantly increased, consistent with an increase in CBS activity. Plasma glutathione levels were significantly reduced in the children with DS and may reflect an increase in oxidative stress due to the overexpression of the superoxide dismutase gene, also located on chromosome 21. The addition of methionine, folinic acid, methyl-B(12), thymidine, or dimethylglycine to the cultured trisomy 21 lymphoblastoid cells improved the metabolic profile in vitro. The increased activity of CBS in children with DS significantly alters homocysteine metabolism such that the folate-dependent resynthesis of methionine is compromised. The decreased availability of homocysteine promotes the well-established "folate trap," creating a functional folate deficiency that may contribute to the metabolic pathology of this complex genetic disorder.
My comments:
First, some information on biochemistry is useful to understand this paper. Folate is important as it helps us synthesize DNA. Here's a simplified view of the folate metabolism cycle:
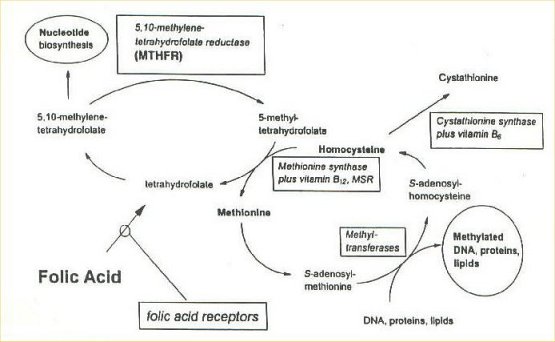
This is simplified beacuse there are really 15 different folate pathway enzymes. (See here for a more complete diagram.)
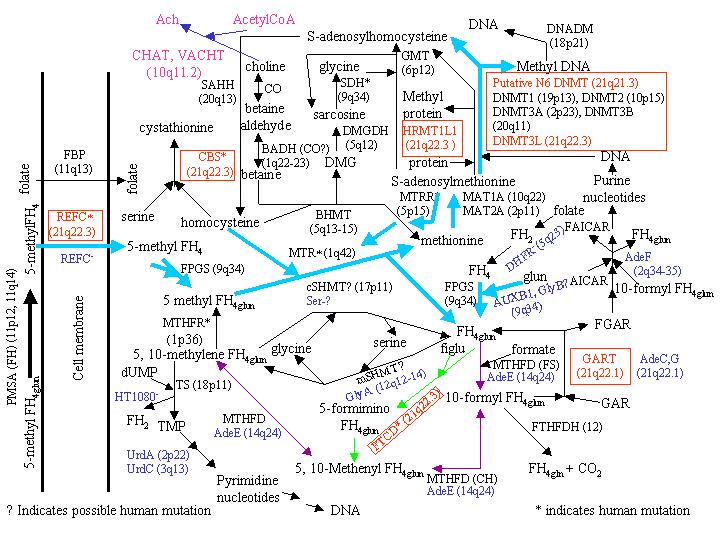{kind=link}
Why should we be worried about folate metabolism in people with DS? For some time, there have been hints that there have been problems with the folate pathway in DS. Specifically, children with DS who require the drug methotrexate for treating leukemia have shown to be very sensitive to this drug, which interferes with folate metabolism. Second, children with DS tend to have larger than normal red blood cells, which may also be an indication of folate difficulties. Dr. Jerome Lejune, who discovered that Down syndrome was due to trisomy of the 21st chromosomes, believed that high doses of folinic acid (a version of folate) would help overcome these metabolic difficulties.
The discovery that the gene that produces the enzyme cystathione synthetase (see the diagram above for this part) sits on the 21st chromosome seemed to indicate that this could be the reason for possible folate problems in DS. This enzyme converts the amino acid homocysteine to the compound cystathionine. If there is an increase in the gene producing this enzyme, then there could be an increase in the enzyme and then more homocysteine would be diverted to make cystathionine, thus reducing the amount available to be converted into the amino acid methionine. If there's less methionine, then there would be less methyl groups made, which would interfere with DNA synthesis.
The problem with these theories was that they were more speculation than fact. Just because a gene is on the 21st chromosome doesn't mean it has an effect in Down syndrome, and to date the studies looking for increased expression of the cystathione synthetase gene showed mixed results. Also, studies of folate supplementation have not proven successful in the past. This study attempts to shed more light on the folate cycle in children with DS.
The first part of the study measured levels of different compounds of the folate cycle. The results of most of the blood tests were in agreement with the theory of more homocysteine going to cystathionine and less methionine being made. However, the study found increased methylated DNA instead of decreased amounts, so it appears that the body has compensated appropriately. It should be noted that at least one other study looked at amino acid levels in people with DS and did not find the differences that this study found. Since both studies appeared to use correct methodology, I can't call the above study conclusive. However, I can report that at least one other research group will be looking hard at the folate cycle in DS, so hopefully we will soon be able to settle this controversy.
The second part of the study involved treating white blood cells from children with DS with supplements outside the body ("in vitro"). As per the authors' expectations, adding certain compounds in the folate cycle increased the amounts of compounds that are made later in the cycle. The authors state that because of this finding, studies are needed to see if oral nutrient supplementation could affect folate metabolism in children with DS. It's important to note that in vitro studies are not useful in making recommendations for nutritional supplementation, since the body has a much more complex environment than the lab dish's environment.
Finally, if the theory is correct that Down syndrome produces a "functional folate deficiency," what would that mean to tbe person with DS? Folate deficiency in children causes larger than usual red blood cells, sometimes with anemia and sometimes without; decreased appetite, inflammation of the tongue, diarrhea, decreased functioning of the immune system and neurologic abnormalities such as depression (but not mental retardation). Of these symptoms, only the findings of large red blood cells and decreased immune system is noted in children with DS, so it doesn't appear that a folate deficiency makes up a large part of the DS condition.
On a related note, the French biochemist P. Kamoun has hypothesized that the problem may instead be excess cysteine (from increased levels of cystathionine) being converted into excess hydrogen sulfide, causing a toxic effect on neurons. He has shown an increased amount of urinary sulfide compounds in people with DS, and is currently researching hydrogen sulfide levels in the blood of children with DS.