Musculoskeletal Disorders in
Down Syndrome
by Len Leshin, MD, FAAP
Copyright 2003, All rights reserved

Almost all of the conditions that effect the bones and joints of people with Down syndrome arise from the abnormal collagen found in Down syndrome. Collagen is the major protein that makes up ligaments, tendons, cartilage, bone and the support structure of the skin. One of the types of collagen (type VI) is encoded by a gene found on the 21st chromosome. The resulting effect in people with DS is increased laxity, or looseness, of the ligaments that attach bone to bone and muscle to bone. The combination of this ligamentous laxity and low muscle tone contribute to orthopedic problems in people with Down syndrome. While these conditions are more common in people with DS than in the general population, it is worthwhile to note that the majority of people with DS will not have any of the disorders I'm discussing in this essay.
In this essay, I'll discuss conditions categorized by body sections.
Spine
The major condition associated with the spine in Down syndrome is Atlantoaxial instability, which is the looseness between the first and second vertebrae of the neck. I have more information on this condition in a separate essay on my website.Another condition associated with the spine in Down syndrome is scoliosis, which is the curvature of the spine to the side. While it appears to be more common in people with DS, the exact incidence isn't known. In the era when almost all children with DS were institutionalized, scoliosis may have been seen in up to half of them as they became adolescents. Treatment of scoliosis remains the same as in other children, with bracing being the initial therapy, followed by surgical intervention if necessary.
Hip
| Five to eight percent of children with DS will develop abnormalities of the hip. The most common condition is dislocation of the hip, which is also called subluxation. In this condition, the head of the thigh bone (the femur) moves out of the socket formed by the pelvis (the acetabulum). This dislocation may or may not be associated with malformation of the acetabulum. The dislocation appears to be due to a combination of laxity of the connective tissue that normally keeps the hip together along with the low muscle tone found in DS. Interestingly, hip subluxation in children with Down syndrome is hardly ever found at birth but instead is most common between the ages of 3 and 13 years. The most common sign is a limp, and pain may or may not be present. Treatment will often start with immobilization of the hip with a cast. Many children with DS will require surgical correction, however. | 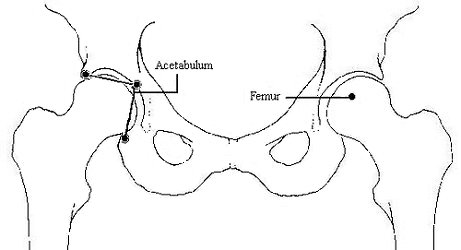 |
Another disorder of the hip is Legg-Calve-Perthes (LCP) disease, in which the head of the femur loses its blood supply and the bone becomes weak and misshapen. LCP is slightly more common in children with DS than in the general population. This condition usually shows up as a painless limp and loss of full range of movement of the involved hip, and is diagnosed through X-rays. Mild cases or cases discovered early may be treated with a combination of bedrest, orthotics and casting. Severe cases require surgical correction.
Slipped capital femoral epiphysis (SCFE, also called "epiphysiolysis") can be seen in people with DS less frequently. In this condition, the rounded head of the femur slides on the neck of the femur. This condition can be associated with obesity and hypothyroidism, both of which are common in teenagers with DS. SCFE appears as a limp with associated pain in the hip or knee (hip conditions often cause knee pain instead of hip pain), and is treated by surgical placement of screws in the femur.
Knee
Instability of the patella (kneecap) has been estimated to occur in close to 20 percent of people with DS. The majority of cases of instability present only as kneecaps that can be moved further to the outside than the normal kneecap (subluxation); however, some people can have their kneecaps completely move out of position (dislocation), and some may even have a hard time getting it back into the right position. Mild subluxation of the kneecap is not associated with pain, but dislocation may be painful. While people with instability of the patella are able to walk, there is often a decreased range of motion of the knee, with an accompanying change in gait. The longer that nothing is done for the instability, the worse the condition will get over time. Orthoses (special braces) may be useful for mild cases, but severe cases require surgical correction.Foot
Flat foot, also called pes planus, is seen in the vast majority of people with DS. In mild cases, the heel is in a neutral position. In severe cases, the heel rotates so that the person is walking on the inside of the heel. Flat feet result in heavy calluses of the feet, pointing of the front part of the feet away from each other (the opposite of being "pigeon-toed"), and even the creation of bone spurs in the feet. Many cases respond to orthotics, but severe cases need surgical correction.| Metatarsus primus varus is also commonly seen in people with DS, and is the condition in which the front part of the foot behind the big toe bends inward. (In this picture, it's the foot on the right that has the problem.) This creates an obvious deformity of the foot, making the task of finding shoes that fit more difficult. If the condition exists long enough, a painful irritation called a bunion appears at the spot where the foot bends in the most. Mild or early cases of the varus may be treated with orthotics or special shoes, but severe cases require surgical correction. | 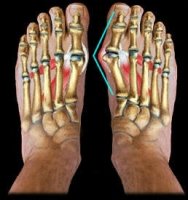 |
Arthritis / Arthropathy
Arthritis refers to the inflammation of a joint which causes pain and swelling of the joint. Arthropathy refers to non-inflammatory disease of a joint, which may have many different causes. There certainly is a higher incidence of joint problems in people with DS, but whether or not there is an increase in the incidence of auto-immune arthritis (such as juvenile rheumatoid arthritis, or JRA) is still being debated in the medical community. One researcher recommended a new condition be named as "Arthropathy of Down syndrome" since the diagnosis of juvenile rheumatoid arthritis is a diagnosis of exclusion (that is, when you make sure that no other disease process is causing the arthritis, then JRA is all you have left). Most researchers, however, are willing to diagnose JRA in children and teens with DS if the specific criteria are met. The treatment of arthritis in people with DS is the same as in people without DS.If the joint pains are not inflammatory in origin, then the most likely cause in people with DS is the hypermobility of the joints. Other causes may also include psoriasis and gout. Doctors who specialize in arthritis and arthropathies are called rheumatologists, and you can find a directory of US and international rheumatologists at http://www.rheumatology.org/directory/geo.asp, including pediatric rheumatologists.
Bones
A small number of studies have indicated that bone density in adults with DS is lower than in the general population, thus increasing the risk for osteoporosis in adulthood, especially of the spine. It is not yet known if supplemental calcium intake will increase bone density in adults with DS. Bone density has not yet been studied in children with DS. Regardless, there is no evidence that children with DS have more broken bones, and likewise there is no evidence that bones in children or adults with DS take longer to mend.
References
- Orthopedic disorders in patients with Down's syndrome. Diamond LS et al. Ortho Clinics North Amer, 12(1):57-71, 1981.
- The hip joint in Down's syndrome. Shaw ED & Beals RK. Clin Ortho Rel Res 278:101-107, 1989.
- Management of dislocation of the hip in Down syndrome. Aprin H, Zink WP, Hall JF. J Ped Ortho 5:428-431, 1985.
- Instability of the patellofemoral joint in Down syndrome. Dugdale TW & Renshaw TS. J Bone Joint Surg 68-A(3):405-413, 1986.
- "Musculoskeletal Disorders." Pueschel SM & Solga PM, in Biomedical Concerns in Persons with Down Syndrome,Brookes Pub Co, 147-157, 1992.
- Arthropathy of Down syndrome. Olson JC et al. Pediatrics 86(6):931-936.